All published articles of this journal are available on ScienceDirect.

The Impact of Psychoeducation on Intolerance of Uncertainty and Psychological Problems among Caregivers of Children with Autism
Authors Info & Affiliations
Abstract
Background
Autism is a neurodevelopmental disorder that severely impacts children and their caregivers. Families, especially parents, caring for children with autism face substantial physical, mental, and social difficulties. Children with autism are more likely to develop anxiety and other mental health issues.
Methods
This study aimed to investigate the impact of a psychoeducational intervention on intolerance of ambiguity and symptoms of mental health difficulties in caregivers of children with autism. A quasi-experimental research design was used. From the Zagazig University Hospital child psychiatric outpatient clinic, a convenience sample of 25 caregivers who accompanied their autistic children receiving therapy in the study settings was obtained. Further, sociodemographic questions, the Intolerance of Uncertainty Scale, and the Depression Anxiety Stress Scales (DASS-21) were used.
Results
The result indicated that the caregivers were mostly female (72%), with a mean age of 39.92±8.96 years and a range of 26 to 55 years old. Most of the children were below the age of 10, with a mean±SD of 9.43±3.46, with the disease duration ranging from 1.7 to 12 years. About 36% of them had a concomitant disease with autism. Meanwhile, over half of them got mental or behavioral treatments (52%), while 48% received speech therapy. From pre- to post-intervention, there were significant reductions in caregivers’ intolerance of uncertainty and symptoms of depression, anxiety, and stress.
Conclusion
A psychoeducational intervention significantly reduced caregivers’ intolerance of uncertainty and symptoms of mental health difficulties. Training nurses and clinical psychologists to administer effective stress management techniques, for example, through a nurse-led parent-to-parent support group, could be integral to reducing stress and anxiety in caregivers.
1. INTRODUCTION
Autism Spectrum Disorder (ASD) is a neurological and developmental disorder that impacts behaviour, learning, communication, and connection with others. An autism diagnosis can be made at any age, though symptoms typically manifest in the first two years of life [1]. Individuals with autism have specific needs and abilities, which may change over time. While some autistic individuals can live independently, others have significant difficulties doing so and require care and support throughout their lives. Autism frequently affects opportunities to pursue further education and employment. The families of people with autism often face substantial difficulty providing sufficient care and support [2].
Intolerance of uncertainty (IU) is defined as the inability to deal with the undesired cognitive, affective, and behavioural consequences of a perceived lack of information. Overvaluation of predictability and a tendency to be overwhelmed by unexpected or unknown events are key characteristics of IU. The construct encompasses ‘inhibitory IU’, which reflects difficulty with current uncertainty and can manifest as freezing in unpredictable situations, and ‘prospective IU’, which reflects anxiety about future events and manifests as a need for predictability [3]. IU has been acknowledged as a dispositional risk factor for generalized anxiety disorder [4].
The entire family is affected when a child has autism, and the condition can be costly, time-consuming, and upsetting. Parenting an ASD child can be difficult and stressful, more so in nations that have limited access to support resources. It is, therefore, important to consider the mental and physical well-being of the whole family. Parents of children with ASD often report poor mental health, including depression and anxiety, reduced quality of life, low well-being, and elevated stress. Previous studies suggest that mothers of children with ASD experience heightened psychological distress and caregiving burden in addition to health issues, low resilience, and difficulties across a range of aspects of family life aspects [5].
The term ‘psychoeducation’ refers to a broad strategy that involves the provision of knowledge and information regarding psychological conditions and treatment approaches. Comprehensive psychoeducation programs help to provide a healthy home setting through promoting effective communication, problem-solving abilities, and coping mechanisms. Strengthening these abilities and strategies increases the likelihood of caregivers effectively managing the conditions of those in their care [6, 7]. For families with a child who has autism, psychoeducation can help deal with the condition and its consequences together, in turn lessening concerns about the child and empowering family members to make educated treatment decisions. Randomized controlled studies show that parenting training improves autistic children’s communication skills, reduces maternal depression, and increases mothers’ understanding of autism and communication styles [8]. The previous research suggested that healthcare officials and nurses should assist those parents by providing them with counseling, training, and support as they adjust to caring for autistic children. Mothers whose children have autism might benefit from an educational program that incorporates techniques to build resilience [8].
1.1. Aims and Hypothesis
The aim of the current study is to assess the influence of a psychoeducational intervention on intolerance of uncertainty and psychological difficulties among caregivers of children with autism. We hypothesize that the intervention will lead to significant reductions in intolerance of uncertainty and psychological difficulties.
2. METHODS
2.1. Design and Setting
The study followed a one-group quasi-experimental design with pre-post evaluation. It was conducted at Zagazig University Hospital’s child psychiatric outpatient clinic, which is the study investigators’ place of work. The hospital serves patients from various socioeconomic and educational backgrounds from regions surrounding Zagazig City. This location and institution were selected based on their convenience for the researchers and accessibility of data.
2.1.1. Sample Size
The impact of a psychoeducation program on intolerance of uncertainty among autism caregivers showed a 50% reduction (from 70% to 20%), with a confidence level of 95% on two sides and the power of study at 90%. The calculated sample size was 25 caregivers.
2.1.2. Participants
We recruited a convenience sample of 25 caregivers who accompanied their autistic children receiving therapy. Inclusion criteria were that caregivers could read and write in Arabic, had been the primary caregivers of a child with autism for at least one year, and that the child had received therapy in the research setting. Caregivers who were illiterate, those who declined or withdrew from participation, and those who failed to attend sessions regularly were excluded.
2.1.3. Measures
Participants completed a self-administered questionnaire that included the Intolerance of Uncertainty Scale (IUS-12) and the Depression Anxiety Stress Scale (DASS-21). A sociodemographic and clinical data sheet was also given to collect information about caregivers’ gender, age, marital status, social status, education, occupation, number of children, and monthly income. Data on autistic children included age, length of diagnosis, comorbid conditions, forms of treatment received, and compliance with follow-up.
2.2. Intolerance of Uncertainty Scale
The 27-item Intolerance of Uncertainty Scale [9] was designed in Quebec to gauge responses to ambiguity and uncertainty. An English version of the measure was developed by Buhr and Dugas (2002), followed by an abbreviated 12-item version [10]. The scale uses a Likert scale response format ranging from 1 (not at all like me) to 5 (completely like me). Items make up two factors [10, 11]: IU-prospective comprises seven items related to future events (e.g., “I cannot bear being taken by surprise”), while IU-inhibitory comprises five items and assesses avoidant responses to ambiguity. Both factors show a high internal consistency of α =.85 [10]. The IUS-12 significantly correlates with the full scale (r =.94 to 96) and shows a continuous latent structure [10, 12, 13]. In this study, the scale demonstrated satisfactory reliability with a Cronbach's α coefficient of 0.76. We used a 50% cutoff to distinguish low versus high intolerance of uncertainty.
2.3. Depression Anxiety Stress Scales 21
The Depression Anxiety Stress Scales 21 (DASS-21) are used to measure emotional states experienced in the previous week [14]. The questionnaire comprises three 7-item subscales and uses a 4-point Likert response format, ranging from 0 = not applicable to 3 = highly applicable [15]. Mean scores for each subscale were computed. The extent of depression, anxiety, and stress was assessed based on the following ranges: < 0.6 = normal, 0.6–1.2 = mild, 1.2–1.8 = moderate, 1.8–2.4 = severe, 2.4–3 = extremely severe). We used the Arabic version with no changes (Moussa et al., 2017). A recent Jordanian study found that Cronbach's α coefficients for three subscales were 0.89 for depression, 0.89 for anxiety, and 0.91 for stress [16]. In this study, Cronbach's α for the full scale was 0.90, and subscales were 0.81 for depression, 0.814 for anxiety, and 0.799 for stress
2.4. Procedure
The study was conducted from August to November 2023 and proceeded in four phases: assessment, planning, execution, and evaluation.
2.4.1. Assessment
Researchers met with caregivers in the study setting to discuss the research purpose and methods. Those who wished to participate gave their informed consent and were given the questionnaire and instructions on how to complete it. Responses provided baseline data for later comparison and allowed researchers to determine caregivers’ learning requirements and tailor the intervention accordingly. Caregivers completed the forms on-site with researchers present to clarify any misunderstandings.
2.4.2. Planning
Researchers scrutinized the pre-test data before formulating the intervention aim, specific objectives, session timing plan, and teaching approaches. The researchers produced a guidebook, titled ‘The Impact of Psychoeducation Intervention on the Intolerance of Uncertainty and Psychological Problems among Caregivers of Children with Autism’ in plain Arabic to accommodate the level of attending caregivers. The guidebook was developed in collaboration with a clinical psychologist to ensure the efficacy of the program. It was informed by an analysis of up-to-date and pertinent literature, with material selected based on caregivers’ indicated needs. The guidebook provided important information for caregivers of ASD children, including ASD definitions, causes, signs and symptoms, diagnosis, nutrition, treatment, children’s needs, and guidance about how to cope and relate with children. The clinical psychologist provided guidance regarding appropriate relaxation techniques for the caregivers.
2.4.3. Implementation
We provided psychoeducation programs to teach caregivers of autistic children how to reduce resistance to unpredictable everyday situations. There were eight sessions, each lasting 45–60 minutes. Session materials were created collaboratively among the research team. Caregivers were assigned to groups of five. Sessions were delivered once per week to each group. Each session had a title and aim that coincided with its content.
2.4.3.1. Session 1
The researcher welcomed and thanked the caregivers for participating in the sessions and discussed general aims and guidelines, such as the meeting location and the weekly agenda. Pre-test data were collected.
2.4.3.2. Session 2
This session provided a comprehensive overview of autism, incorporating prevalence, common symptoms, etiology, information on early diagnosis, available therapy, prognosis, and the role of parents in treatment.
2.4.3.3. Session 3
The aim of this session was to teach mothers how to gauge and guide their children’s behaviour and choose appropriate games and activities.
2.4.3.4. Session 4
The goal of this session was to teach participants about identifying and modifying behavioural problems. It also included information on educational resources and social games.
2.4.3.5. Sessions 5-6
These sessions focused on family communication skills and methods. They included how to establish rapport with children, what to do if a child becomes angry or demanding, and how to use calming reinforcement approaches. They also provided advice on problem-solving and resources.
2.5. Evaluation
We examined the impact of the intervention on participants’ intolerance of uncertainty and mental health by using the same questionnaire used in the pre-test.
2.6. Pilot Study
To evaluate our questionnaire’s intelligibility and ascertain the time required to complete it, we conducted a pilot study with 10% of the caregivers who met the inclusion criteria. No modifications were required based on piloting. We removed pilot survey data from the research results. The questionnaire was written in clear, self-explanatory language and required 15–20 minutes to complete. Five specialists in child mental medicine and psychiatric health nursing confirmed the Arabic-translated questionnaire’s content validity. An assessment of test-retest reliability indicated that all scales were acceptable.
2.7. Ethical Considerations
The Zagazig University Faculty of Nursing Research Ethics Committee approved the study and gave permission to proceed (ID/Zu.Nur.REC #:72). The administration of Zagazig University Hospital also granted permission after being informed about the study’s purpose and procedures. The researchers followed all ethical guidelines outlined in the Helsinki Declaration. Caregivers were informed their participation was completely voluntary and that they could withdraw their participation at any time without consequence. We guaranteed the confidentiality and anonymity of all data acquired and assigned codes to identify participants in our analysis. Each participant provided a written authorization form before completing the questionnaire.
2.8. Statistical Analysis
Data were analysed using SPSS version 20.0 for Windows (SPSS Inc., Chicago, IL, USA). Quantitative data were reported as means and standard deviations, while qualitative data were presented as numerical values and percentages. Paired ordinal data were subjected to the marginal homogeneity test. Pairwise categorical data were analysed using the Mcnemar test. The association between variables was examined using the Pearson correlation coefficient. Each test was two-sided. We used an alpha level of p < 0.05 for significance testing. We calculated improvement scores with the following formula: % of improvement = (post-intervention value – pre-intervention value) / pre-intervention value * 100.
3. RESULTS
Table 1 presents the sociodemographic characteristics of the sample. Caregivers in the study were aged 26–55 years old (M = 39.92 ± 8.96) and were mostly female (72%). Most were married (92%) and had either secondary (44%) or university (36%) education. Over half were housewives (56%), and just over half reported an insufficient monthly income (52%).
| Variable | n | % |
|---|---|---|
|
Age in years Mean ± SD Median (range) |
39.92 ± 8.96 38 (26–55) |
|
| < 40 years ≥ 40 years |
13 12 |
52.0 48.0 |
| Gender | ||
| Male | 7 | 28.0 |
| Female | 18 | 72.0 |
| Social status | ||
| Married | 23 | 92.0 |
| Divorced | 2 | 8.0 |
| Education | ||
| Read and write | 4 | 16.0 |
| Basic education | 1 | 4.0 |
| Secondary school | 11 | 44.0 |
| University | 9 | 36.0 |
| Employment status | ||
| Employed | 10 | 40.0 |
| Not Working | 1 | 4.0 |
| Housewife | 14 | 56.0 |
| Number of children | ||
| 1 | 2 | 8.0 |
| 2 | 8 | 32.0 |
| 3 | 7 | 28.0 |
| 4 | 7 | 28.0 |
| 5 | 1 | 4.0 |
| Income | ||
| Enough | 12 | 48.0 |
| Insufficient | 13 | 52.0 |
Table 2 presents the clinical characteristics and demographic information of the children with autism included in the study. Most were below age 10 (M = 9.43 ± 3.46), with duration since diagnosis ranging from 1.7 to 12 years. About 36% had a concomitant condition with autism. Over half received mental or behavioural treatment (52%), while 48% received speech therapy.
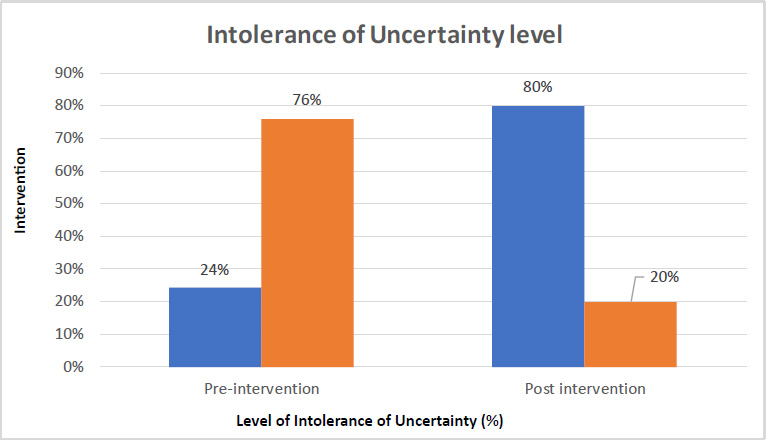
In terms of uncertainty intolerance, Table 3 displays a statistically significant improvement in overall (IUS) mean scores from M±SD 36.44±8.1 in the preintervention phase to M±SD19.76±7.93 post-intervention. Also, there was a statistically significant decrease in prospective IU mean scores in the pre-intervention from ±SD 20.32±5.14 to M±SD 12.56±4.89 post-intervention. Similarly, the mean inhibitory subscale scores in the studied sample reduced considerably from M±SD14.12±3.64 in the preintervention phase to M±SD7.12±3.76 in the post-intervention phase, with (p <0.05); this illustrates the worth of psychoeducational intervention in reducing feelings of uncertainty.
Fig. (1) shows levels of intolerance of uncertainty, split into low and high with a 50% cutoff, before and after the intervention. We found that 76% of caregivers had high IUS before the intervention. This figure dropped to 20% after the intervention.
| Variable | n | % |
|---|---|---|
|
Age in years < 10 years ≥ 10 years |
15 10 |
60.0 40.0 |
| Mean ± SD Median (range) |
9.43 ± 3.46 8.8 (4.11–16.0) |
|
|
Disease duration in years Mean ± SD Median (range) |
6.24 ± 3.64 6 (1.7–12) |
|
| Comorbid condition (yes/no) | 9 | 36.0 |
| Other children in the family have autism (yes/no) | 0 | 0.0 |
| Receiving treatment (yes/no) | 19 | 76.0 |
|
Types of Treatment • Pharmacological treatment • Psychiatric or behavioral treatment • Speech treatment • Pharmacological and speech treatment • Pharmacological, psychiatric, and behavioral treatment |
9 13 12 7 7 |
36.0 52.0 48.0 28.0 28.0 |
| Commitment to follow-up | - | - |
| Not at all | 1 | 4.0 |
| Always | 24 | 96.0 |
| Variable | Caregiver Intolerance of Uncertainty | % Improvement | p-value | |||||
|---|---|---|---|---|---|---|---|---|
|
Pre-intervention (n = 25) |
Post-intervention (n = 25) |
|||||||
| n | % | n | % | |||||
| Prospective IU | ||||||||
| Low | 10 | 40.0 | 18 | 72.0 | - | 0.46 | ||
| High | 15 | 60.0 | 7 | 28.0 | 43.11 | - | ||
| Mean ± SD Median (range) |
20.32 ± 5.14 19 (9–29) |
12.56 ± 4.89 13 (7–22) |
||||||
| Inhibitory IU | ||||||||
| Low | 5 | 20.0 | 20 | 80.0 | - | .001 | ||
| High | 20 | 80.0 | 5 | 20.0 | - | - | ||
| Mean ± SD Median (range) |
14.12 ± 3.64 14 (6–21) |
7.12 ± 3.76 8 (5–18) |
49.58 | - | ||||
| Total IU | ||||||||
| Low | 6 | 24.0 | 20 | 80.0 | - | 0.001 | ||
| High | 19 | 76.0 | 5 | 20.0 | 45.77 | - | ||
| Mean ± SD Median (range) |
36.44 ± 8.1 35 (15–48) |
19.76 ± 7.93 22 (12–35) |
||||||
Impact of intervention on intolerance of uncertainty among caregivers of children with autism.
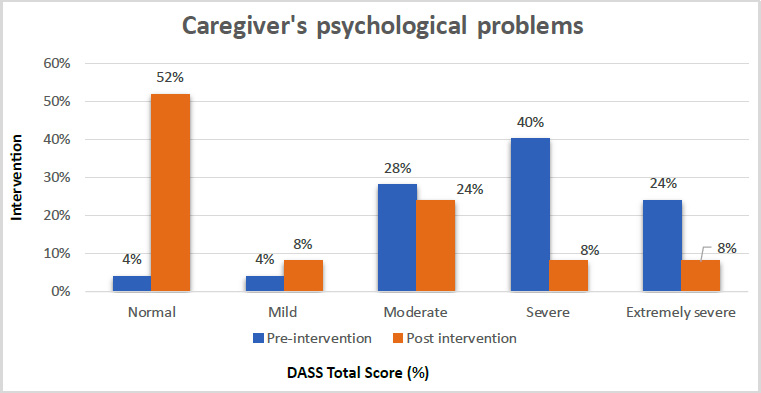
Table 4 shows DASS scores before and after the intervention. We observed a statistically significant decline in mean depression scores, from M = 9.64 (± 4.82) before the intervention to M = 4.88 (± 4.55) after. Preintervention, extremely severe anxiety, and stress were reported by 56% and 32% of the sample, respectively. There were significant decreases in anxiety scores, from M = 10.88 (± 4.86) before the intervention to M = 6.64 (± 4.09) after, and stress scores, which fell from M = 12.84 (± 4.46) before the intervention to M = 6.4 (± 4.85) after. There were also statistically significant decreases in overall DASS scores, from M = 36.36 (± 12.03) before the intervention to M = 15.76 (± 12.89) after. These results suggest that the intervention was successful in reducing symptoms of depression, anxiety, and stress.
Fig. (2) shows percentages of DASS total scores before and after the intervention. Before the intervention, 64% reported symptoms in the severe or extremely severe range. This proportion fell to 16% after the intervention. The proportion scoring in the normal range increased from just 4% to over half the sample (52%).
Table 5 presents correlations between study variables, showing that intolerance of uncertainty and its two subscales were significantly positively associated with DASS depression, anxiety, and stress subscales. There were also positive associations between both DASS and IUS and the child’s age, number of children, and disease duration. Caregiver age negatively correlated with DASS and IUS, but these correlations were not significant.
Impact of intervention on caregiver dass scores by symptom severity.
| Variable | Caregivers’ Depression, Anxiety, and Stress Symptoms | % Improvement | p-value | |||||
|---|---|---|---|---|---|---|---|---|
|
Pre-intervention (n = 25) |
Post-intervention (n = 25) |
|||||||
| n | % | n | % | |||||
| Depression | ||||||||
| Normal | 4 | 16.0 | 15 | 60.0 | - | 0.01 | ||
| Mild | 2 | 8.0 | 0 | 0.0 | - | - | ||
| Moderate | 11 | 44.0 | 7 | 28.0 | - | - | ||
| Severe | 3 | 12.0 | 1 | 4.0 | - | - | ||
| Extremely severe | 5 | 20.0 | 2 | 8.0 | 49.38 | - | ||
| Mean ± SD Median (range) |
9.64 ± 4.82 9 (1–20) |
4.88 ± 4.55 4 (0–15) |
||||||
| Anxiety | ||||||||
| Normal | 2 | 8.0 | 3 | 12.0 | - | 0.002 | ||
| Mild | 0 | 0.0 | 4 | 16.0 | - | - | ||
| Moderate | 3 | 12.0 | 11 | 44.0 | - | - | ||
| Severe | 6 | 24.0 | 3 | 12.0 | - | - | ||
| Extremely severe | 14 | 56.0 | 4 | 16.0 | 38.97 | - | ||
| Mean ± SD Median (range) |
10.88 ± 4.86 10 (2–21) |
6.64 ± 4.09 6 (0–16) |
||||||
| Stress | ||||||||
| Normal | 4 | 16.0 | 16 | 64.0 | - | 0.001 | ||
| Mild | 4 | 16.0 | 1 | 4.0 | - | - | ||
| Moderate | 4 | 16.0 | 4 | 16.0 | - | - | ||
| Severe | 5 | 20.0 | 4 | 16.0 | - | - | ||
| Extremely severe | 8 | 32.0 | 0 | 0.0 | 50.16 | - | ||
| Mean ± SD Median (range) |
12.84 ± 4.46 13 (5–20) |
6.4 ± 4.85 4 (1–15) |
||||||
| DASS | 0.0001 | |||||||
| Normal (0-30) | 1 | 4.0 | 13 | 52.0 | - | |||
| Mild (31-40) | 1 | 4.0 | 2 | 8.0 | - | |||
| Moderate (41-59) | 7 | 28.0 | 6 | 24.0 | - | |||
| Severe (60-79) | 10 | 40.0 | 2 | 8.0 | - | |||
| Extremely severe (80+) | 6 | 24.0 | 2 | 8.0 | 56.7 | |||
| Mean ± SD Median (range) |
36.36 ± 12.03 34 (9–59) |
15.76 ± 12.89 15 (2–46) |
||||||
| Variable | DASS | Intolerance of Uncertainty | ||
|---|---|---|---|---|
| r | p | r | p | |
| Intolerance of Uncertainty (Total) | 0.650** | 0.0001 | - | - |
| Stress | 0.655** | 0.0001 | ||
| Depression | 0.645** | 0.0001 | ||
| Anxiety | 0.598** | 0.002 | ||
| IU-Inhibitory | 0.463* | 0.02 | ||
| IU-Prospective | 0.711** | 0.0001 | ||
| Caregiver’s age | -0.024 | 0.908 | -0.069 | 0.742 |
| Child’s age | 0.123 | 0.557 | 0.107 | 0.61 |
| Number of children | 0.056 | 0.79 | 0.345 | 0.091 |
| Diagnosis duration | 0.154 | 0.462 | 0.114 | 0.588 |
4. DISCUSSION
The results of this study show that our psychoeducational intervention led to a significant reduction in intolerance of uncertainty as well as decreased symptoms of depression, anxiety, and stress in caregivers of autistic children. These findings support our research hypothesis.
The caregivers in our sample were representative of patients in government hospitals in Egypt. Most were married women, more than a third had a university education, and over half had more than three children. The high percentage of female caregivers resonates with findings that women are more likely than men to take primary responsibility for caring for relatives generally, particularly for children with ASD and ADHD [17]. Furthermore, a recent Saudi Arabian poll found that more than one-third of the mothers examined had a university degree [18].
The majority of children with autism in the study were under age 10, while around a third had a concomitant condition. Over half had received psychiatric, behavioural, or speech therapy. As such, our sample represented children diagnosed with autism at an early age and requiring multidisciplinary treatment approaches. Previous studies confirm that comorbidity is common in those with autism [19]. Indeed, one study of autistic children found that caregivers faced substantial hurdles when children were aged four to eight due to an increased likelihood of comorbidity and more pronounced emotional or behavioural symptoms [20]. Psychological and behavioural treatments, as well as psychiatry, are common therapeutic approaches for problematic, dysfunctional behaviours linked with ASD, such as hyperactivity, anxiety, and self-injury [21, 22].
Our baseline measures revealed that a substantial majority of caregivers in the study reported a high intolerance of uncertainty before the intervention. Having a child diagnosed with autism and responding to the behavioral, emotional, and psychological manifestations of the condition understandably produces intense anxiety and uncertainty about the child’s future. The condition can be perceived as a complex issue that is difficult to tackle and, therefore, a threat to the child’s well-being. Likewise, a lack of sufficient information about the child’s illness can exacerbate caregivers’ intolerance of uncertainty. Our findings are consistent with those of a previous study, which concluded that intolerance of uncertainty was associated with a perceived lack of necessary information [23]. Moreover, previous findings indicate that parents of children with autism spectrum disorder demonstrate a high intolerance for uncertainty and suffer fear and worry due to the unpredictability of their children’s condition [24-26]. An inability to respond effectively to uncertainty is linked to poor coping mechanisms and psychological maladaptation [27]. In addition, a recent study suggested that intolerance to prospective uncertainty particularly increased worry, while inhibitory intolerance to uncertainty was related to negative coping, which contributed to anxiety and depression symptoms [28].
We observed a statistically significant reduction in the overall intolerance of uncertainty and the prospective and inhibitory subscales from pre- to post-intervention, supporting the intervention’s effectiveness. The intervention was designed to address various concerns and needs of this group of caregivers, including social and psychological support, accurate information, behavioural management advice, and service navigation. Notably, intolerance of uncertainty and its subscales showed strong positive relationships with depression, anxiety, and stress symptoms after the intervention.
Our findings are consistent with an earlier study carried out with caregivers of schizophrenia patients, which showed that psychoeducational interventions were effective at reducing uncertainty, increasing optimism, and promoting the seeking of social support [29]. Another study using an uncertainty-focused psychoeducation program also found a substantial reduction in intolerance of uncertainty and an indirect impact on reduced anxiety and depression symptoms after a four week follow-up [29]. Such family-centered approaches to overcoming uncertainty-related difficulties are effective and valuable [30].
A large proportion of participants in the study reported extremely severe anxiety and stress before the intervention, as well as moderate depression. This could be attributed to the experience of caring for an autistic child. The high percentage of negative emotions in this sample implies the need for interventions that tackle the mental health concerns of caregivers. Encouragingly, there was a significant drop in mean depression, anxiety, and stress scores over the intervention, showing that our intervention was effective in lessening symptoms of mental difficulties. These findings bolster a recent study of autistic preschool children’s families, which showed reduced parenting stress after a psychoeducation program up to six months after the intervention finished. These findings and ours highlight the value of psychoeducation in addressing caregivers’ needs, especially if interventions are delivered at an early stage. Relatedly, a study conducted in Saudi Arabia found that psychoeducation was useful in improving parental well-being among mothers of autistic children [31]. There may, however, be ceiling effects on the positive impact of such interventions [32].
4.1. Limitations
One weakness of this study is that it only examined the effect of a sole psychoeducational intervention on intolerance of uncertainty and emotional difficulties in caregivers of autistic children, with no control group. The relatively small sample size limits the generalizability of our findings. Furthermore, we only looked at short-term impacts, with no long-term follow-up. A longer-term assessment would reveal whether the effects of the intervention are long-lasting and sustainable.
CONCLUSION
Evidence from this study showed that caregivers for children with autism reported high intolerance of uncertainty, severe anxiety and stress, and moderate depression at baseline. An eight-week psychoeducation intervention led to significant reductions in scores on all of these variables. Our data support the beneficial effect of this psychoeducational intervention in improving the mental health and well-being of caregivers.
RECOMMENDATIONS
Further studies should investigate the advantages of including other relatives in psychoeducation to improve family well-being more broadly. There should also be consideration of other personal resources that could eliminate strain on parents, perhaps through enhancing coping skills to improve the psychological resilience of caregivers.
Training nurses and clinical psychologists to administer effective stress management techniques, for example, through a nurse-led parent-to-parent support group, could be integral to reducing stress and anxiety in caregivers.
AUTHORS’ CONTRIBUTIONS
R.M.H. and B.A.A.: Conceived and designed the study; K.M.A., N.R.A., R.M.H., and B.A.A.: Prepared the intervention program; K.M.A. and N.R.A.: Performed the statistical analyses; R.M.H. and B.A.A.: Edited and drafted the paper; B.A.A. and N.R.A.: Participated in data collection. All authors provided input regarding the manuscript and approved the final version.
LIST OF ABBREVIATIONS
| ASD | = Autism Spectrum Disorder |
| DASS-21 | = Depression Anxiety Stress Scales 21 |
| IU | = Intolerance of Uncertainty |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The Zagazig University Faculty of Nursing Research Ethics Committee, Egypt approved the study and gave permission to proceed (ID/Zu.Nur.REC #:72).
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Caregivers were informed their participation was completely voluntary and that they could withdraw their participation at any time without consequence.
AVAILABILITY OF DATA AND MATERIALS
The datasets examined in this investigation can be retrieved from the corresponding author [K.A].
ACKNOWLEDGEMENTS
The authors would like to thank all caregivers of autistic children who agreed to participate in the study.