All published articles of this journal are available on ScienceDirect.

Effectiveness of Demonstration-based Educational Sessions on Management of Chest Tube Drainage among Nurses
Authors Info & Affiliations
Abstract
Introduction
Chest tube drainage system is to restore intra-pleural negative pressure and to promote the re-expansion of the lungs. However, if it is not managed properly, it can lead to complications.
Aim
Current study aimed to assess and evaluate the nurse’s knowledge and practices regarding the management of chest tube drainage at public hospital and to improve it through demonstration-based educational sessions.
Methods
A quasi-experimental study design was exploited to evaluate the effectiveness of Demonstration based educational sessions on the management of chest tube drainage among nurses. A total of 58 nurses participated in the study via Simple Random Sampling technique.
Results
Pre-Knowledge of nurses was found to be poor; none of the participants obtained a good knowledge score. While the post-test knowledge scores were significantly improved to the good category after the demonstration based educational sessions.
Conclusion
The demonstration based educational session was effective for the improvement of nurse’s knowledge.
1. INTRODUCTION
Chest trauma is the third most common cause of death around the world, accounting for 25% of all traumatic deaths. There are many lung pathologies like chest trauma, pneumothorax, empyema, chylothorax, and hydrothorax that warrant the insertion of a chest tube and a drainage system to drain air, blood, pus, or lymph from the pleural cavity, thereby restoring proper ventilation. Chest tube drainage consists of a hollow flexible tube, which at one end is inserted into the pleural space and the other end attached to a drainage system. The drainage system includes a suction source, a collection chamber for pleural drainage, and a one-way valve.
Chest tube insertion is a crucial intervention in cardiothoracic surgery, chest trauma, and blunt traumas. In the United States of America (USA), every year, more than 300,000 patients undergo cardiothoracic surgery requiring the placement of at least one chest tube. Blunt traumas cause more than 150,000 deaths in Europe per year. Among them, around 18% of patients require a chest drain. Approximately 16,000 deaths per year in India occur as a result of chest trauma. Among them 90% of the patients are managed by insertion of chest tubes. However, meticulous care is required in the management of chest tube drainage because improper management may lead to various complications. A study demonstrated that poor management of chest tube drainage was associated with complications like lung infection (32.9%), pneumothorax (17.7%), bleeding (13.5%), pleural effusion 8.4%, and septicemia (6.3%).
Nurses’ knowledge regarding the care of patients with chest tube drainage plays a paramount role in the prevention of associated complications. However, the results of different studies have revealed that nurses had unsatisfactory knowledge related to chest tubes. Studies in Pakistan have also shown knowledge deficit and improper management of chest tube drainage, which leads to multiple complications.
There is a paucity of research regarding educational sessions' effectiveness in handling chest tubes among nurses; hence this study is being designed to address this knowledge gap. Study findings may have implications for providing safe and effective care of chest tube drainage [1-15].
1.1. Aim of the Study
The study aims to assess and evaluate the nurse’s knowledge and practice regarding the management of chest tube drainage at Saidu Group of Teaching Hospital (SGTH) and to improve nurses’ knowledge and practice through demonstration-based educational sessions.
2. MATERIALS AND METHODS
2.3. Sample Size
The sample size for the study was calculated through a G-Power sample size calculator with a power of 0.95, an alpha error of 0.05, and an effect size of 0.5. The sample size given by G-Power was (n=54), but with 10% non-respond rate, the total number of study participants selected for the study was 60.
2.3.1. Sample Selection
The total number of nurses working in the three departments was 113. The proportion-based selection was made from the three departments. The participants from Intensive care units were: (39/113*60=21), Surgical departments: (59/113*60=31), Pulmonology departments: (14/113*60=08), (21+31+08 = 60). The names of the participants were printed on different pages separately, and a lottery method was used to carry out the study among the total population.
2.3.2. Sampling Technique
Simple random sampling technique was brought into consideration for the selection of the participants.
2.4. Instruments of the Study
2.4.1. Questionnaire
The questionnaire was adopted from Dr. Sabah Abbas Ahmad.
2.4.1.1. Validity & Reliability
The validity of the instrument was checked through 14-panel experts who were faculty members from the College of Nursing and Surgeons. For the reliability of the questionnaire, she conducted a pilot study on 10 nurses in which she determined the reliability of the instruments, which was statistically significant with an alpha correlation coefficient of (r = 0.78) [14].
2.4.1.2. Questionnaire Consists of Four Sections
- Demographic characteristics of nurses.
- Knowledge of nurses regarding chest anatomy, indication and contraindication of chest tube, and chest tube drainage system (18Mcqs).
- Knowledge of Nurses regarding a nursing role in the insertion and removal of a chest tube. (15 true and false items).
- Knowledge of Nurses regarding nursing intervention for chest tube drainage system. (15 true and false items).
2.5. Practical Demonstration
A practical demonstration was provided to the study participants so that they may learn how to practically perform a procedure.
2.6. National Health Services (NHS) Guidelines for Chest Drain
National health services (NHS) are considered to be the heart of England. It provides services of ensuring the provision of quality care. These guidelines (chest drains guidelines for the insertion and management in adults) were first approved in 2017.
2.7. Ethical Permissions
Ethical permission was obtained from Ethical Review Committee of Khyber Medical University, Reference Number of the committee was (No. Dir/KMU-EB/ED/ 000955). Moreover, informed consent was obtained from each of the participants independently. Privacy and confidentiality were ensured while handling the participant’s information.
2.8. Data Analysis Procedure
The analysis of the data was carried out through descriptive statistics and inferential statistics.
The data was coded and transferred to the coding sheet. After that the data was entered into SPSS (version 26) and finally, analysis and interpretation of data were carried out.
3. RESULTS
In the current study, the gender composition of the participants was found equally as 28 (50%) male, and 28 (50%) were female. According to the age of the participants, 3.4% of participants were in the age category of 20-25 years, 43.1% were in the age category of 26-30 years, 34.5% were in the age category of 31-35 years, 13.8 were in the age category of 36-40, and 5.2% were above 40 years of age. According to the study findings regarding the educational status reveal that 39.7% were General Nursing Diploma holders, 37.9% had post-RN degrees, which is a two-year degree after General Nursing Diploma, while 22.4 had Generic BSN degrees. The findings of the study revealed that 5.20% had an experience of 1-2 years, 27.60% were in the category of 3-5 years, 46.60% were in the category of 6-10 years, and 17.2% were in the category of 11-15 years, while 3.40 were having an experienced of 16 and above years. In the current study, 30 participants were selected from surgical departments, 20 from intensive care units, and 08 were selected from the pulmonology department. The demographic characteristics were presented in Table 1 for a better understanding.
| - | Frequency | Percent | Valid Percent | Cumulative Percent | |
|---|---|---|---|---|---|
| Gender | Male | 29 | 50.0 | 50.0 | 50.0 |
| Female | 29 | 50.0 | 50.0 | 100.0 | |
| Age | 20-25 | 2 | 3.4 | 3.4 | 3.4 |
| 26-30 | 25 | 43.1 | 43.1 | 46.6 | |
| 31-35 | 20 | 34.5 | 34.5 | 81.0 | |
| 36-40 | 8 | 13.8 | 13.8 | 94.8 | |
| Above 40 | 3 | 5.2 | 5.2 | 100.0 | |
| Qualification | Diploma | 23 | 39.7 | 39.7 | 39.7 |
| Generic BSN | 13 | 22.4 | 22.4 | 62.1 | |
| Post RN | 22 | 37.9 | 37.9 | 100.0 | |
| Experience | 1-2 years | 3 | 5.2 | 5.2 | 5.2 |
| 3-5 years | 16 | 27.6 | 27.6 | 32.8 | |
| 6-10 years | 27 | 46.6 | 46.6 | 79.3 | |
| 11-15 years | 10 | 17.2 | 17.2 | 96.6 | |
| 16 years and above | 2 | 3.4 | 3.4 | 100.0 | |
| Departments | Surgical department | 30 | 51.7 | 51.7 | 51.7 |
| ICU | 20 | 34.5 | 34.5 | 86.2 | |
| Pulmonology | 8 | 13.8 | 13.8 | 100.0 | |
| Participation before | No | 58 | 100.0 | 100.0 | 100.0 |
3.1. Pre- and Post-Test Mean Difference Score
In the comparison of pre- and post-mean knowledge scores (Fig. 1), results showed a pre-mean score of (7.77±2.55, 7.89±1.59, 7.67±1.91) respectively in all three sections. In the post-mean score, it was (13.82±3.26, 11.98±1.87, and 11.93±2.13) respectively in all three sections. Similarly, the difference between the pre and post knowledge score in percentages had been determined, which was stated in figures for better understanding. Figures 2-4 showed the mean percentage difference in score before and after the research intervention.

Comparison of mean difference between pre and post knowledge score.
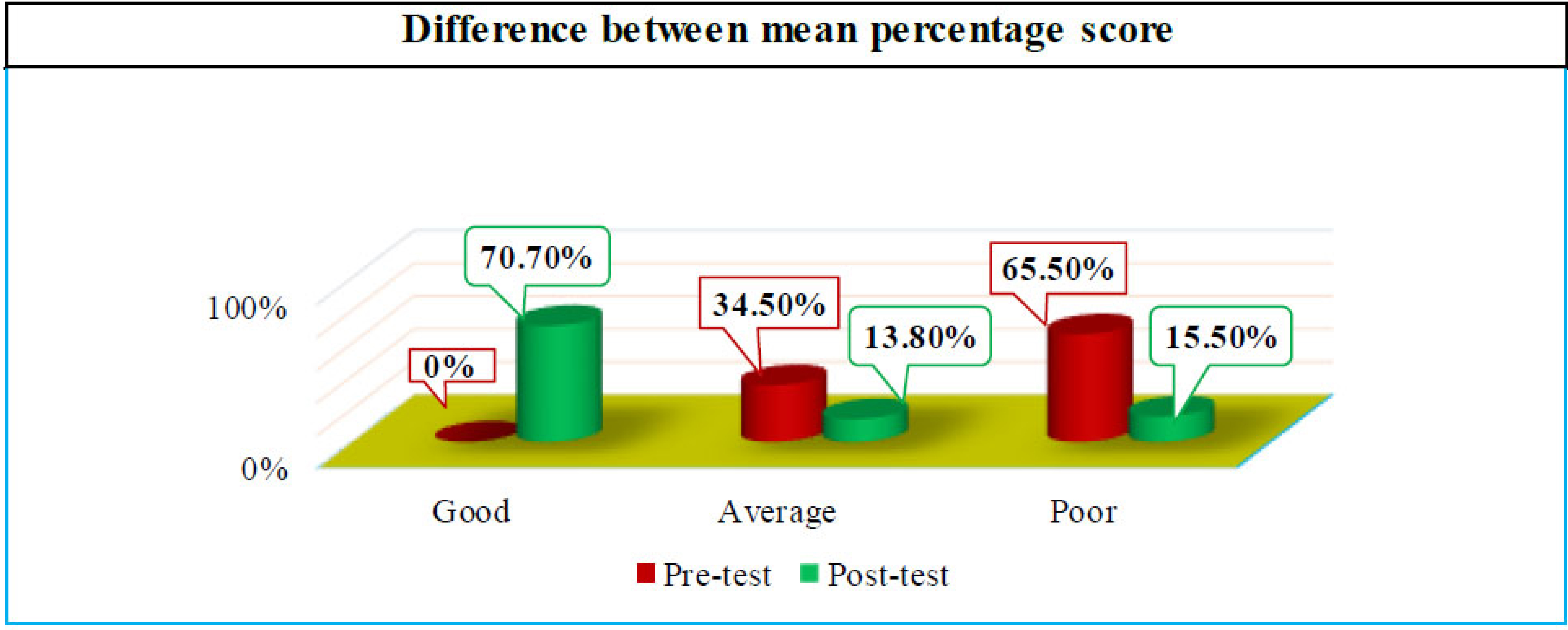
Nurses' knowledge regarding basics of chest anatomy and chest tube.
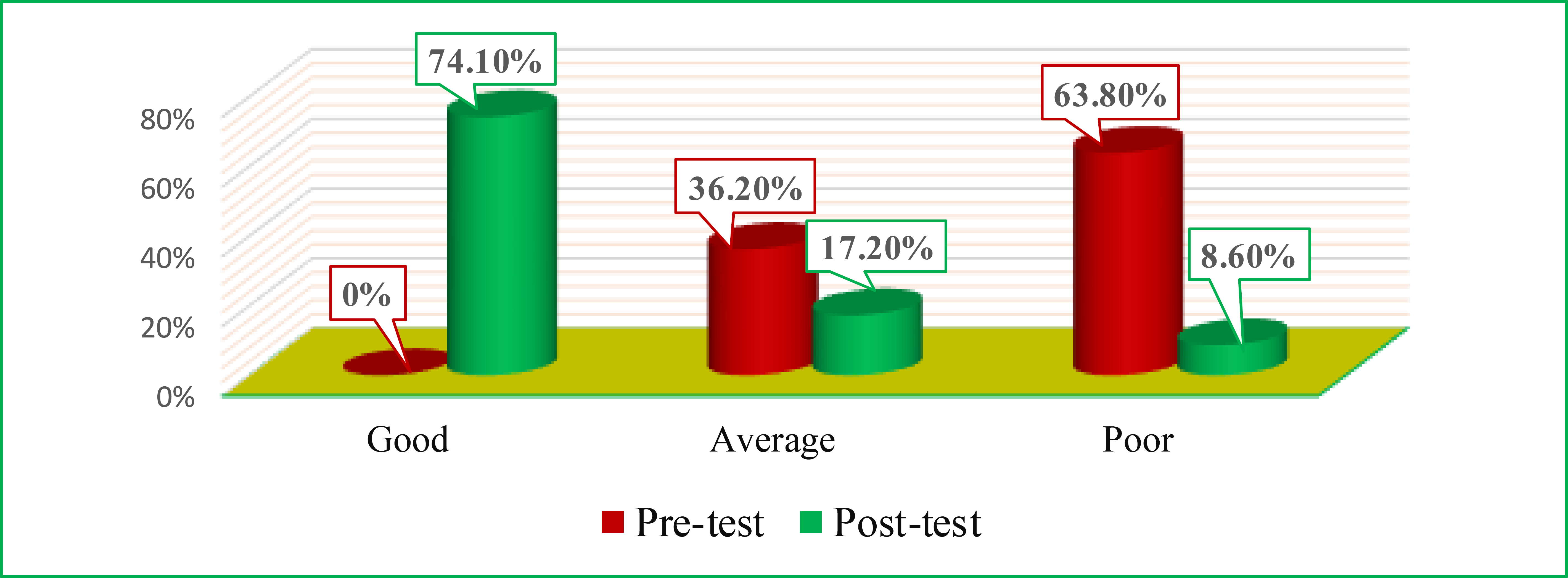
Nursing role in the insertion and removal of chest tube and drainage.
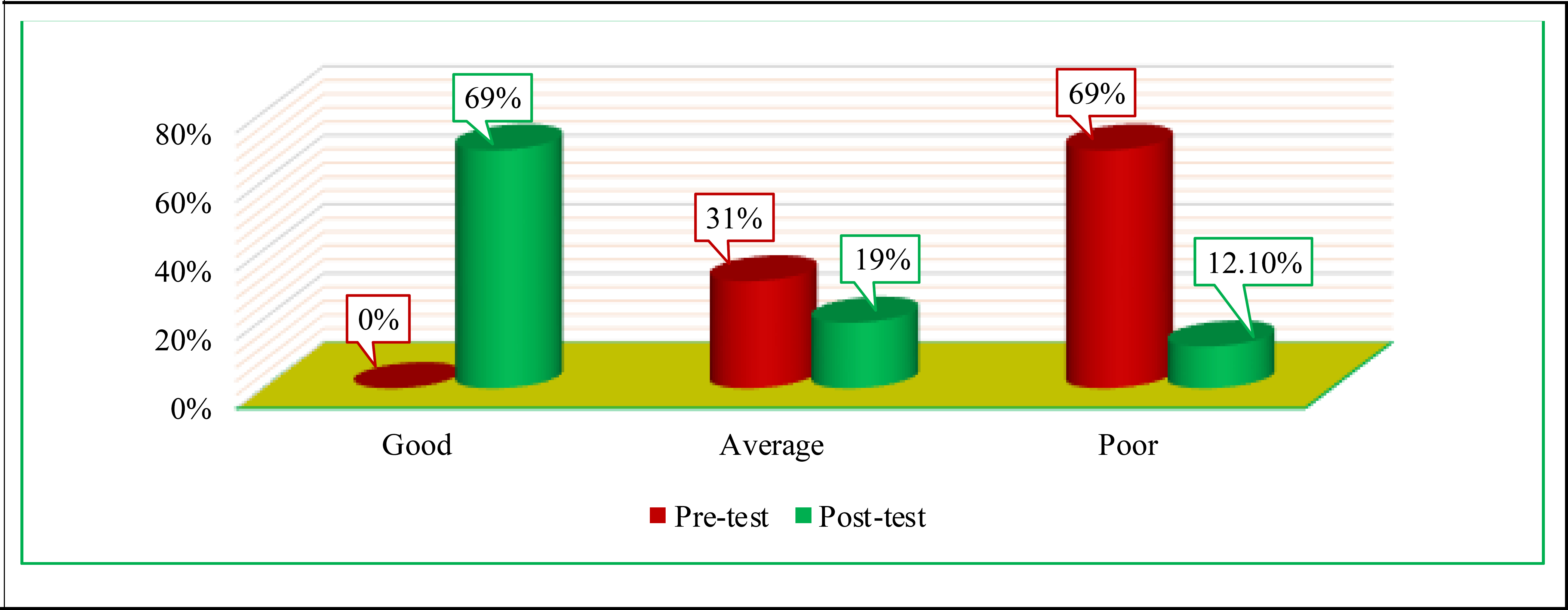
Nurses' knowledge regarding nursing intervention of chest tube drainage.
3.2. Paired Sample t-test
The paired t-test was also applied to calculate the mean difference. The application of paired t-test was to evaluate the effectiveness of demonstration-based Educational Sessions. The difference in mean scores among all three paired with pre-and post-knowledge was (-6.051, -4.086, -4.258), with a standard deviation (SD) of (±3.69, ±1.940, ±2.148) as shown in Table 2.
| - | Paired Differences | t | df | Sig. | |||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | Std. Deviation | Std. Error Mean | 95% Confidence Interval of the Difference | ||||||
| Lower | Upper | ||||||||
| Pair 1 | Pre- and Post- knowledge score | -6.051 | 3.696 | 0.485 | -7.023 | -5.079 | -12.468 | 57 | 0.000 |
| Pair 2 | Pre-nurse role CAT, Post nurse role | -4.086 | 1.940 | 0.254 | -4.596 | -3.576 | -16.039 | 57 | 0.000 |
| Pair 3 | Pre- and Post- nursing intervention | -4.258 | 2.148 | 0.282 | -4.823 | -3.693 | -15.095 | 57 | 0.000 |
3.3. Association between the Pre-test Knowledge Score with Selected Demographic Variables
Association of pre knowledge score was analyzed through chi-square test. Pre-knowledge score was evaluated with selected demographic variables, as shown in Tables 3-5.
| - | Association of pre-knowledge score with the age | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre-knowledge CAT | ||||||||||||||||
| Poor | Average | df | Chi-square | p-value | ||||||||||||
| Age | 20-25 | 2 | 0 | 4 | 0.269 | NS | ||||||||||
| 26-30 | 17 | 8 | ||||||||||||||
| 31-35 | 11 | 9 | ||||||||||||||
| 36-40 | 7 | 1 | ||||||||||||||
| above 40 | 1 | 2 | ||||||||||||||
| - | Pre-nurse role CAT | |||||||||||||||
| Poor | Average | df | Chi-square | p-value | ||||||||||||
| Age | 20-25 | 1 | 1 | 4 | 0.387 | NS | ||||||||||
| 26-30 | 13 | 12 | ||||||||||||||
| 31-35 | 14 | 6 | ||||||||||||||
| 36-40 | 6 | 2 | ||||||||||||||
| above 40 | 3 | 0 | ||||||||||||||
| - | Pre-nursing intervention CAT | |||||||||||||||
| Poor | Average | df | Chi-square | p-value | ||||||||||||
| Age | 20-25 | 2 | 0 | 4 | 0.588 | NS | ||||||||||
| 26-30 | 16 | 9 | ||||||||||||||
| 31-35 | 13 | 7 | ||||||||||||||
| 36-40 | 6 | 2 | ||||||||||||||
| above 40 | 3 | 0 | ||||||||||||||
| - | Association of pre-knowledge score with an experience | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre-knowlege CAT | ||||||||||||||||
| Poor | Average | df | Chi-square | p-value | ||||||||||||
| Experience | 1-2 years | 2 | 1 | 4 | 0.900 | NS | ||||||||||
| 3-5 years | 12 | 4 | ||||||||||||||
| 6-10 years | 17 | 10 | ||||||||||||||
| 11-15 years | 6 | 4 | ||||||||||||||
| 16 years and above | 1 | 1 | ||||||||||||||
| - | Pre-nurse role CAT | |||||||||||||||
| Poor | Average | df | Chi-square | p-value | ||||||||||||
| Experience | 1-2 years | 0 | 3 | 4 | 0.090 | NS | ||||||||||
| 3-5 years | 9 | 7 | ||||||||||||||
| 6-10 years | 18 | 9 | ||||||||||||||
| 11-15 years | 8 | 2 | ||||||||||||||
| 16 years and above | 2 | 0 | ||||||||||||||
| - | Pre_Nursing_Intervention_CAT | |||||||||||||||
| Poor | Average | df | Chi-square | p-value | ||||||||||||
| Experience | 1-2 years | 1 | 2 | 4 | 0.275 | NS | ||||||||||
| 3-5 years | 10 | 6 | ||||||||||||||
| 6-10 years | 18 | 9 | ||||||||||||||
| 11-15 years | 9 | 1 | ||||||||||||||
| 16 years and above | 2 | 0 | ||||||||||||||
| - | Association of pre-knowledge score with the qualification | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre-knowledge CAT | ||||||||||||||||
| Poor | Average | df | Chi-square | p-value | ||||||||||||
| Qualification | Diploma | 19 | 4 | 2 | 0.00 | NS | ||||||||||
| BSN | 4 | 9 | ||||||||||||||
| Post-RN | 15 | 7 | ||||||||||||||
| - | Pre-nurse role CAT | |||||||||||||||
| Poor | Average | df | Chi-square | p-value | ||||||||||||
| Qualification | Diploma | 18 | 5 | 2 | 0.00 | NS | ||||||||||
| BSN | 2 | 11 | ||||||||||||||
| Post-RN | 17 | 5 | ||||||||||||||
| - | Pre-nursing intervention CAT | |||||||||||||||
| Poor | Average | df | Chi-square | p-value | ||||||||||||
| Qualification | Diploma | 20 | 3 | 2 | 0.01 | Sig. | ||||||||||
| BSN | 5 | 8 | ||||||||||||||
| Post-RN | 15 | 7 | ||||||||||||||
4. DISCUSSION
The gender composition shows that 50% of the participants in the current study were female while 50% were male. These findings are quite contradictory to the results of many studies in which 100% of the participants were female. Similarly, another study's results revealed that the gender composition of the participants was 93.3% females and 6.6% males [11]. Likewise, another study result showed that 81% of participants were female and 19% were male [16, 17]. The result of the study findings had shown that the majority of the participants were from the age of 26-30 (43.10%), followed by 31-35 (34.50%), 36-40 (13.80%), above 40 were (5.20%) and 20-25 were (3.40%). These findings are similar to a study, in which the majority of the participants (63.3%) were in the age group between 20-25 years (Ibrahim, 2014) [8]. Similarly, another study result showed that the majority of the participants (48.7%) were in the age group of 26-30 years (Health, 2018) [7]. The distribution of the participants regarding qualification shows that the majority of the subjects were General Nursing Diploma holders (39.70%), followed by post-RN 37.90%, and then BScN (22.40%). The findings of the current study are similar to a study in which more than half of the participants (60%) were having a General Nursing Diploma, while only 6% of the participants were BSN degree holders [17]. In another study, 80% of the participants were diploma holders and 20% had technical education [12]. Similarly, another study's findings revealed that 70% of the participants had a Nursing diploma and 30% had technical institute training (Ibrahim, 2014) [8]. Distribution according to the experience of the participants shows that the majority of the participants (46.60%) were having an experience of 6-10 years, followed by 27.60% (3-5 years), 17.20% (11-15 years), 5.20% (1-2 years), and 3.40% were having an experience of 16 years and above. These findings are contradictory to a study's findings in which the majority of the participants (36.67%) had experience of (1-5 years) while 16.67% had (6-10) years of experience [15]. Likewise, in another study, the result showed that 38.6% of the participants had an experience of more than 05 years, while 45.5% had an experience of 1-5years (Elfaki et al., 2016). The results are contradictory to a study's findings in which 36.6% were fresh nurses with an experience of 1-5 years while only 16% had an experience of 6-10 years [14]. The pre-mean score of participants in knowledge regarding basics was 7.77. The score in the nursing role in the insertion and removal of chest tube was (7.89). Correspondingly, in the Nursing Intervention section, the score was (7.67). The pre-mean knowledge score of the participants in all three sections falls under the category of poor knowledge. In the post-test mean knowledge scores were, knowledge regarding basic was (13.82), in nursing role in the insertion and removal of chest tube was (11.98), while in nursing intervention it was (11.92). These findings are analogous to study results in which the pre-knowledge mean score was (15.88), while the post-session mean score obtained was (25.18) [11]. Similarly, in another study, the result revealed a pre-knowledge mean score of (13.20) and the post-knowledge mean score of (23.0) [15]. To determine nurses' knowledge in different categories, the variables pre-knowledge score and post knowledge score were categorized into three different categories. These categories were poor, average, and good knowledge scores based on bloom cut-off value, as mentioned in the methodology section of the study. The results indicated that (65.50%) participants obtained poor scores, (34.50%) scored average, and none of the participants achieved a good score in the knowledge of basic chest anatomy and chest tube drainage system section. In the same way, the second section, “nurse's role in the insertion and removal of chest tube” (63.80%), scored poor, (36.20%) scored average and none of the participants obtained a good knowledge score. In the third section, “nursing intervention” regarding chest tube drainage (69%), respondents scored poor, (31%) reached an average score and none of the participants obtained a good score. These results of the current study are comparable to the findings of a study in which 40% of the participants in the pre-test scored poorly, 50% obtained an average knowledge score and 10% obtained a good knowledge score [15]. Similarly, another study result showed that 46.7% scored poorly while 43.3% obtained an average score [16]. Furthermore, another study results had shown that 75.7% had unsatisfactory knowledge scores regarding different aspects of chest tube drainage [12]. Moreover, a study had shown highly insignificant results in which (100%) of the participants had shown unsatisfactory knowledge scores [9, 12]. These identical results could be due to nurses' lack of personal interest in gaining and implementing their theoretical knowledge in their clinical practice. After the implementation of the intervention, the post-knowledge score was re-assessed. The results showed that 70.70% of the participants obtained a good knowledge score, almost (14%) of the participants scored average, and (15%) respondents scored poor in the knowledge of chest anatomy and chest tube section. Correspondingly, in the second section of the questionnaire nursing role in the insertion and removal of chest tube drainage [74.10%] participants scored good, [17.20%] participants scored average, and only [8.60%] participants obtained poor scores. Likewise, in the third section nurse's knowledge regarding nursing intervention on chest tube drainage (69%) participants scored good, (19%) scored average, and only (12%) participants obtained poor scores. Similarly, in the comparison of pre and post-test knowledge scores via paired t-test, there is a highly significant difference of (0.000) in all three sections respectively. These findings are similar to the result of a study in which there is a highly significant difference of (0.000) [8]. Similarly, another study's results had also revealed a highly significant association of (0.000) among pre and post-test score comparisons [14]. Thus, the result of the current study showed that demonstration-based educational session was highly productive for the participants and also showed significant improvement in the post-knowledge score.
5. LIMITATION
- The current study was a mandatory part of MS-Nursing Degree the first limitation was time bound restriction to be completed in 06 months. This hindered recruitment of participants from the Multiple setup and diverse categories of hospitals in the province.
- The resource for the demonstration and management of chest tube drainages was the second restraint in the study. It was a self-funded research work.
CONCLUSION
The current study was an interventional study that was purely designed to provide a benefit to nurses in the form of provision of interventions on the management of chest tube drainage. According to the study findings, the majority of the participants (43%) were of age 26-30 years, and a maximum of the participants (46%) had an experience of 6-10 years. In the pre-test, nurses showed poor knowledge of 65.50%, 63.80%, 69% in all three sections of the questionnaire. The post-intervention results showed a significant improvement in the knowledge scores. In the post-intervention, nurses gave knowledge scores of 70.70%, 74.10%, and 69%, respectively. Hence, the Demonstration-based educational sessions were proven effective in the improvement of nurses' knowledge regarding the management of chest tube drainage.
RECOMMENDATION
Based on the study findings, the following recommendations can be drawn:
- A similar study can be conducted by selecting a large number of participants from different hospitals.
- A true-experimental study needs to be conducted with a control group for a better understanding of knowledge and practices regarding chest tube drainage.
- A comparative study can be done among public and private hospitals to explore further gaps in the knowledge and practices.
- Seminars, workshops, and educational sessions can be arranged for the improvement of the nurse's knowledge and practices.
- Proper guidelines and checklist availability can be made assured in the practice areas and can be strictly followed by everyone.
- Nursing educational services must include at in their curriculum as per the National Patient Safety Agency and current study findings.
AUTHORS’ CONTRIBUTIONS
It is hereby acknowledged that all authors have accepted responsibility for the manuscript's content and consented to its submission. They have meticulously reviewed all results and unanimously approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| USA | = United States of America |
| SGTH | = Saidu Group of Teaching Hospital |
| NHS | = National Health Services |
| SD | = Standard Deviation |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval was obtained from the Ethical Review Committee of Khyber Medical University, Pakistan Reference Number of the committee was (No. Dir/KMU-EB/ED/000955).
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
ACKNOWLEDGEMENTS
Declared none.