All published articles of this journal are available on ScienceDirect.

Scoping Review on Challenges and Barriers in Triage Education for Emergency Nurses
Abstract
Introduction/Objective
Triage effectiveness, especially the application of the Canadian Triage and Acuity Scale (CTAS), is vital to patient safety in emergency departments (EDs). The aim of this scoping review was to conduct a systematic literature mapping of knowledge about barriers to triage education among emergency nurses, focusing on the use of CTAS in resource-constrained settings, including Saudi Arabia.
Methods
Based on the Joanna Briggs Institute (JBI) approach to scoping reviews, a comprehensive search using PubMed, Embase, CINAHL, Google Scholar, and OpenGrey to find peer-reviewed literature (2015–2025) was conducted. Eligibility was defined using the Population-Concept-Context (PCC) framework. Thematic synthesis, data extraction, and study selection were performed.
Results
A total of twelve studies met the inclusion criteria. The major obstacles were divided into the following groups: professional (e.g., lack of expertise, error rates of 20–38%), environmental (e.g., noise, overcrowding), and systemic (e.g., absence of standardized training, staffing shortages). Subgroup analysis showed that emerging and inexperienced nurses faced increased challenges, particularly in non-Canadian settings implementing CTAS.
Discussion
Multifaceted interventions are needed due to the interplay of barriers. There is promise in simulation-based learning and standardized curricula. Cultural and infrastructural aspects of certain regions, such as the Qassim region of Saudi Arabia, require customized models such as the Qassim Comprehensive Triage Model (QCTM-CTAS).
Conclusion
Targeted, evidence-based strategies are urgently required to overcome triage education barriers, enhance CTAS proficiency, and improve patient outcomes globally.
1. INTRODUCTION
The emergency departments (EDs) serve as key points of the healthcare system, as the primary triage procedure has a direct impact on patient flow, resource distribution, and clinical outcomes [1]. Triage is effective in ensuring that patients are attended to depending on the urgency of their case. One such tool that has been adopted and validated to standardize this prioritization process is the Canadian Triage and Acuity Scale (CTAS), which is a five-level tool [2]. Nevertheless, sustained, high-quality education and practical training, which are essential in attaining and retaining expertise in the use of CTAS, are often undermined by a complex set of impediments.
These educational problems are put into perspective with the help of theoretical frameworks. The Novice to Expert model by Benner illustrates the developmental process of clinical judgment in triage, and the Pyramid of Clinical Competence by Miller underlines that one should go beyond knowledge and start to act [3, 4]. Moreover, Social Learning Theory emphasizes the impact of organizational culture and interprofessional relations on the process of acquiring and applying skills [5]. Although educational interventions such as simulation-based learning (SBL) have been developed to address the gap between theoretical content and the disorganized reality in the ED, such interventions are often hampered by systemic and resource-related barriers [6].
Such issues are especially acute where healthcare is changing at a high pace. The Qassim region in Saudi Arabia has an ambitious reform agenda in the form of Vision 2030, which intends to modernize health services; however, the EDs are faced with large patient numbers, cultural diversity, and a lack of infrastructural support and empowerment, which is adding to the existing triage education gaps [7, 8]. It is thus important to closely analyze these barriers in this particular context.
This scoping review does not rely on a general enumeration of obstacles. It will attempt to systematically map and synthesize the evidence on triage education barriers among emergency nurses, including CTAS. It has the following specific objectives:
- Outline the reported barriers within professional, environmental, and systemic domains.
- Examine CTAS-specific hurdles, especially in non-Canadian and resource-constrained settings.
- Propose evidence-informed educational strategies and models tailored to address these gaps.
2. METHODS
The Joanna Briggs Institute (JBI) approach to scoping reviews was followed in conducting this scoping review [9]. This approach was used to systematically map the existing literature without undertaking a formal critical appraisal of the included sources, and it focused on the breadth of the evidence.
2.1. Protocol and Eligibility Criteria
The Population-Concept-Context (PCC) framework was used as a guide for the review to establish clear eligibility criteria.
2.1.1. Population
Registered nurses who primarily work in and conduct triage in emergency departments of hospitals. Studies that focused on other healthcare professionals (e.g., physicians, paramedics) or non-ED settings were excluded.
2.1.2. Concept
The context was global EDs, with particular interest in studies that involved the Canadian Triage and Acuity Scale (CTAS) and studies carried out in resource-constrained settings. Only peer-reviewed articles in English were considered, and they must have been published between January 2015 and September 2025. All study designs (qualitative, quantitative, and mixed-methods) were included. Non-peer-reviewed literature (editorials, commentaries, etc.) was excluded.
2.2. Information Sources and Search Strategy
A comprehensive search strategy was developed in collaboration with a health sciences librarian. The following electronic databases were searched to ensure broad coverage of medical, nursing, and allied health literature: PubMed, Embase, and CINAHL. To identify grey literature and mitigate publication bias, Google Scholar (first 200 relevant results) and OpenGrey were also searched.
The search strategy used a combination of Medical Subject Headings (MeSH) and free-text terms related to the PCC elements. Key search terms included “triage,” “emergency nursing,” “Canadian Triage and Acuity Scale,” “CTAS,” “education,” “training,” “barriers,” and “challenges.” Boolean operators (AND, OR) were used to combine terms. The full search strategy for each database is provided in Supplementary File 1.
2.3. Study Selection Process
All records identified were uploaded into Covidence systematic review software to manage them. After duplicates were removed, a two-stage screening process was adopted. First, titles and abstracts were screened independently by two reviewers against the eligibility criteria. Second, full texts of studies that were potentially relevant were retrieved and assessed separately. Any disagreements at any stage were resolved through discussion or by involving a third reviewer. The study selection process is described in the PRISMA-ScR flow diagram (Fig. S1), and reporting compliance is ensured using the PRISMA-ScR checklist (Table S1).
2.4. Data Charting
Two independent reviewers extracted data from the included studies using a standardized, piloted form. The data retrieved included the study author, year of publication, country, study design, sample size, key findings, and barriers to triage education. During extraction, barriers were initially coded as professional (P), environmental (E), or systemic (S). The final data extraction table is provided in Table S2.
2.5. Synthesis of Results
Since the aim of the scoping review was to do so, the theoretical analysis was carried out through narrative synthesis with thematic analysis. The extracted barriers were further broken down through iterative analysis and grouped into coherent themes. The results are presented in a descriptive and visual manner in summary tables to chart the main concepts and evidence.
3. RESULTS
3.1. Study Selection
The PRISMA-ScR flow diagram (Fig. 1) summarises the systematic search and selection process. Database and grey literature searches identified 152 unique records. After title and abstract screening and full-text review, 12 articles met all eligibility criteria and were included for data extraction and synthesis. Compliance with scoping review reporting standards is summarized in the PRISMA-ScR checklist (Table S1).
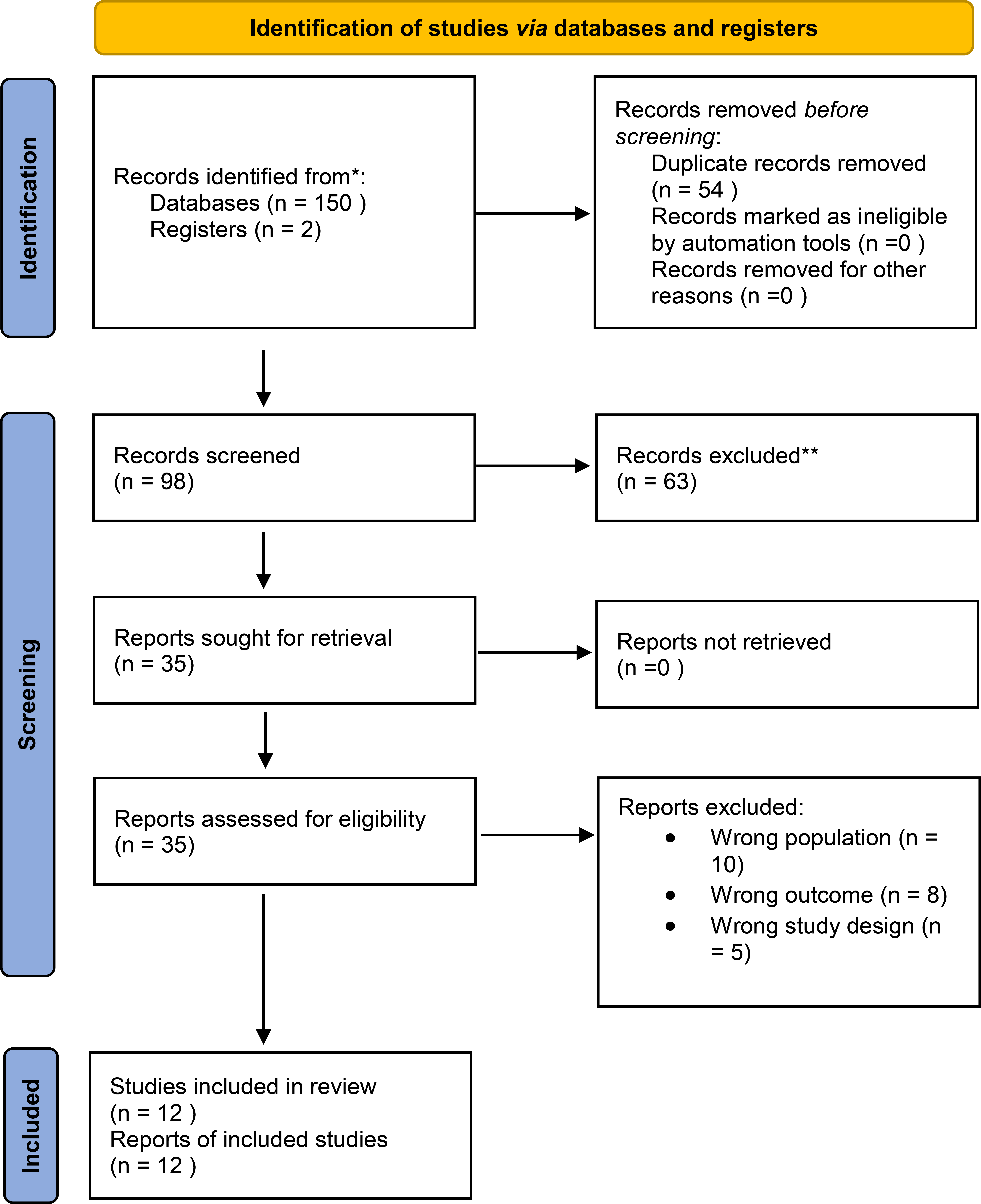
PRISMA-ScR flow diagram illustrating the study selection process: 152 records identified, 98 screened, 35 assessed for eligibility, and 12 included.
3.2. Characteristics of Included Studies
The 12 included studies, published between 2015 and 2025, originated from nine different countries: Canada (n=2), Saudi Arabia (n=2), Iran (n=2), Ethiopia, France, Australia, Ghana, China, and the United States (n=1 each). The study designs included one reliability study, two qualitative studies, two cross-sectional studies, one quasi-experimental study, two mixed-methods studies, and four review-based studies. Sample sizes ranged from 10 to 200 participants in primary studies. The complete data extraction for all studies, including design, sample, and key findings, is available in Table S2. An overview of study characteristics is presented in Table 1.
| Author(s) | Year | Country | Study Design | Sample Size |
|---|---|---|---|---|
| Alquraini et al. [10] | 2015 | Saudi Arabia | Reliability Study | 10 nurses (160 case scenarios) |
| Li et al. [16] | 2018 | China | Meta-analysis | N/A |
| Hardy & Calleja [17] | 2018 | Australia | Scoping Review | N/A |
| Bijani & Khaleghi [14] | 2019 | Iran | Qualitative | 20 nurses |
| Duko et al. [12] | 2019 | Ethiopia | Cross-sectional | 101 nurses |
| Reay et al. [20] | 2019 | Canada | Qualitative | 25 nurses |
| Rosenberg [21] | 2019 | USA | Review | N/A |
| Delmas et al. [15] | 2020 | France | Quasi-experimental | 30 nurses |
| Salifu et al. [13] | 2022 | Ghana | Mixed-methods | 40 nurses |
| Soola et al. [22] | 2022 | Iran | Cross-sectional | 200 nurses |
| Al-Thobaity et al. [11] | 2024 | Saudi Arabia | Mixed-methods | 172 nurses + expert interviews |
| Ouellet et al. [18] | 2025 | Canada | Systematic Review | N/A |
3.3. Synthesis of Barriers to Triage Education
Thematic analysis of the extracted data identified ten key barrier themes, which were categorized into three overarching domains: Professional, Environmental, and Systemic. The mapping of these barriers to the supporting studies is summarized in Table 2.
| Barrier Theme (Domain) | Description | Supporting Studies (Country) |
|---|---|---|
| 1. Insufficient Professional Expertise (P) | Gaps in foundational and CTAS-specific knowledge, particularly among novice nurses, lead to high rates of under- or over-triage. | Bijani & Khaleghi, 2019 [14] (Iran); Duko et al., 2019 [12] (Ethiopia); Al-Thobaity et al., 2024 [11] (Saudi Arabia) |
| 2. Nurse Shortages & High Workloads (S) | Chronic understaffing leads to rushed assessments, burnout, and limited capacity for training. | Rosenberg, 2019 [21] (USA); Li et al., 2018 [16] (China) |
| 3. Environmental Stressors (E) | Chaotic ED conditions (noise, interruptions, overcrowding) that impair cognitive function and decision-making. | Delmas et al., 2020 [15] (France); Bijani & Khaleghi, 2019 [14] (Iran) |
| 4. Lack of Standardized Education (S) | High variability in triage training curricula, duration, and quality leads to inconsistent competency levels. | Hardy & Calleja, 2018 [17] (Australia); Salifu et al., 2022 [13] (Ghana); Ouellet et al., 2025 [18] (Canada) |
| 5. Inadequate Resources & Infrastructure (S) | Absence of dedicated training resources, such as simulation labs or updated technology, to support practical education. | Salifu et al., 2022 [13] (Ghana) |
| 6. Cultural & Communication Barriers (P/S) | Challenges in cross-cultural communication and varying patient perceptions of urgency, especially in diverse populations. | Al-Thobaity et al., 2024 [11] (Saudi Arabia) |
| 7. Lack of Interprofessional Collaboration (S) | Role ambiguity and poor communication between ED nurses, prehospital providers, and other hospital teams. | Reay et al., 2019 [20] (Canada) |
| 8. Misaligned Prehospital-ED Systems (S) | Inconsistencies in triage protocols and information handover between emergency medical services and the ED. | Reay et al., 2019 [20] (Canada) |
| 9. Insufficient Leadership & Policy Support (S) | Absence of institutional prioritization, funding, or formal policies to mandate and sustain triage education programs. | Hardy & Calleja, 2018 [17] (Australia); Salifu et al., 2022 [13] (Ghana) |
| 10. Resistance to Change (P) | Reluctance among staff to adopt new triage protocols or educational methods due to entrenched traditional practices. | Soola et al., 2022 [18] (Iran) |
Note: P=Professional, E=Environmental, S=Systemic.
3.4. Notable Contextual Findings
Subgroup analysis indicated that the combination and intensity of barriers differed by context. Studies from resource-constrained settings (e.g., Saudi Arabia [10, 11], Ethiopia [12], Ghana [13]) frequently reported compounded systemic barriers, including a lack of standardized training and inadequate resources. Furthermore, novice nurses were identified across multiple studies as being disproportionately vulnerable to these barriers, with reported error rates linked to inexperience ranging from 20% to 38% [10, 12, 14].
4. DISCUSSION
This scoping literature review presents evidence from twelve studies to map obstacles affecting the provision of triage education to emergency nurses, with a specific focus on CTAS implementation. The results show that professional, environmental, and systemic factors are closely interrelated and form a compounded issue that impedes the acquisition of triage competency, especially among inexperienced nurses and in resource-limited settings.
The prevalence of professional obstacles, in particular the lack of expertise, with error rates in the range of 20–38% [10, 12, 14], is consistent with Benner’s conceptualization of the novice stage [4]. Without extensive systematized educational activities and experience, novice nurses find it difficult to apply the level of decision-making demanded by CTAS and tend to revert to rule-based decisions, which are inappropriate for the multifaceted presentation of ED cases. This is a more significant gap in non-Canadian settings where CTAS is implemented without culturally and contextually tailored training resources [10, 11]. A counterproductive learning environment is created by environmental barriers, including overcrowding and noise [14, 15]. Such stressors not only affect the cognitive ability needed to conduct triage accurately in real time but also reduce the capacity to effectively engage in further learning, contributing to a cycle of error and burnout [16].
Nevertheless, these frontline obstacles are often rooted in institutional barriers. There is an underlying inconsistency due to the absence of standardized education [13, 17, 18] and insufficient institutional support [13, 17]. Individual competency becomes variable and dependent on personal initiative in the absence of compulsory, high-quality, continuous training programs. This systemic failure is most pronounced in the Qassim province of Saudi Arabia, where, although the healthcare modernization objectives of Vision 2030 [19] are ambitious, EDs are exposed to infrastructural short-comings such as nursing workforce shortages, which restrict mentorship and limit immersive training opportunities such as simulation [13].
To this integrated network of barriers, there is a need to adapt an evidence-based model to suit the context. The proposed Qassim Comprehensive Triage Model (QCTM-CTAS) is based on direct evidence mapping and is intended to address needs in each area:
- To overcome professional knowledge gaps: The model includes a standardized, tiered curriculum based on Miller’s Pyramid, transitioning from knowledge acquisition to application in practice [4, 18].
- To mitigate environmental stressors: It incorporates simulation-based training that replicates high-fidelity, high-stress ED environments, enabling nurses to develop cognitive resilience and decision-making skills in a controlled setting [13, 15].
- To address systemic shortcomings: The model is built on a framework of policy and leadership support that recommends dedicated funding, protected training time, and the development of train-the-trainer courses to ensure sustainability [13, 17]. It also includes cultural competency and interprofessional communication modules to enhance accuracy across different patient populations and during handover [11, 20].
Triage education is a patient safety issue that should be improved ethically. Minimizing the number of errors will help reduce the legal and professional risks to which nurses are exposed and the ethical obligation of beneficence. It is also efficient as a policy approach, since improved triage accuracy will streamline resource allocation and minimize costly delays in critical care.
5. LIMITATIONS
This review has a number of limitations. The scope was limited to publications in the English language, which may have excluded relevant studies published in other languages. Although several databases were used, the over-representation of studies conducted in Middle Eastern and African settings (8 of 12 studies) may have implications for the generalizability of the results to other regions of the world. The inclusion of different study designs, while appropriate for a scoping review, does not allow for conclusive statements on the magnitude of each barrier.
6. FUTURE RESEARCH
Longitudinal designs should be used in the future to assess the long-term efficacy of intervention models such as the QCTM-CTAS. There is also a need to conduct research to develop and test culture-specific triage training tools in different cultural contexts. Lastly, studies on the economic costs and benefits of investing in standardized triage education may provide a strong case for health system policymakers.
CONCLUSION
This scoping review identified ten interrelated themes across professional, environmental, and systemic domains and mapped all available evidence on barriers to triage education among emergency nurses. The results further show that the attainment of competence in CTAS practice is continuously affected by factors such as lack of expertise, disorganized clinical settings, and absence of uniform and standardized training programs. Such issues are particularly pronounced among novice nurses and in resource-limited settings. A complex approach is needed to improve patient safety and triage accuracy. This approach should combine standardized and simulation-based education with strong institutional and policy support, tailored to the specific local requirements of each region, such as those outlined in Saudi Arabia’s Vision 2030.
AUTHORS' CONTRIBUTIONS
The author confirms contribution to the paper as follows: K.A.: Study conception and design, data collection, analysis and interpretation of results, and draft manuscript: F.S.: Visualization. The author reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| CTAS | = Canadian Triage and Acuity Scale |
| ED | = Emergency Department |
| JBI | = Joanna Briggs Institute |
| PCC | = Population–Concept–Context |
| PRISMA-ScR | = Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews |
| QCTM-CTAS | = Qassim Comprehensive Triage Model |
| SBL | = Simulation-Based Learning |
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of this article are available in the Zenodo repository at https://doi.org/10.5281/zenodo.20293492, reference number 20293492.
ACKNOWLEDGEMENTS
Declared none.